Aftercare Isn't Sweetness - It's a Neurochemical Recovery Protocol
Why aftercare is mandatory biological stabilization, not romantic gesture. Explore endorphin withdrawal, autonomic dysregulation, and the science of post-scene recovery protocols.

Why skipping the cooldown is handing your partner a cortisol bomb
The Crash Nobody Warned You About
You just took someone apart for two hours. Impact, restraint, whatever your flavor—you pushed them deep into subspace, watched their eyes go glassy, felt them dissolve into pure sensation. Beautiful. Then the scene ends, you're both tired, and you figure cuddles are optional. Maybe a quick check-in, some water, you head home or roll over and sleep.
Forty-eight hours later, they're a wreck. Weeping for no reason. Bone-deep exhaustion. Flu-like aches. Emotional rawness that feels like the world lost its skin. They text you something like "I don't know what's wrong with me" and neither of you connect it to what happened in that scene.
This is drop. And you caused it. Not because you're cruel—because nobody taught you that aftercare isn't sentiment. It isn't sweetness, romance, or optional emotional labor. It's a neurochemical recovery protocol, and skipping it is like pushing someone out of a moving car because you arrived at the destination.
Scene without aftercare is surgery without a recovery room. You opened someone up. Now you need to close.
The Pattern: What's Actually Happening in Scene
Intense scenes are neurochemical events. Understanding what you're doing to someone's nervous system explains why aftercare isn't optional—it's load-bearing.
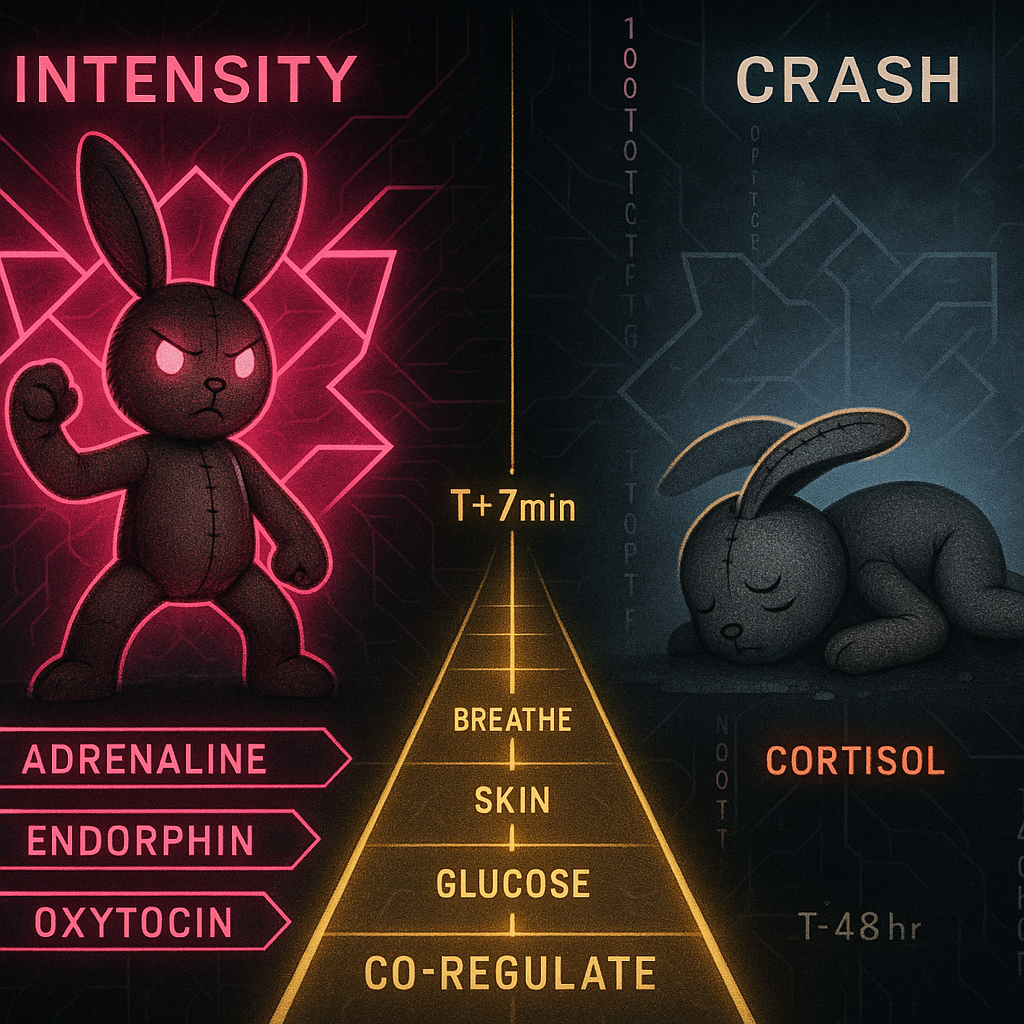
During intensity, the body floods with a cocktail designed for peak performance under stress. Adrenaline sharpens focus. Endorphins kill pain (that's why bottoms can take things in scene they couldn't handle cold). Oxytocin creates bonding and trust. Dopamine drives the reward loop. The nervous system redlines into sympathetic activation—fight-or-flight running hot, held in place by the container of the scene.
This isn't metaphor. Measure someone's heart rate, cortisol, skin conductance during heavy play and you'll see numbers that look like combat or extreme athletics. The body doesn't distinguish between "real threat" and "consensual intensity"—it just sees high arousal plus surrender and responds accordingly.
Then the scene ends. The external stimulation stops. And all those chemicals that were holding the experience together start crashing.
The Mechanism: The Neurochemistry of Drop
Drop is autonomic rebound. It's what happens when the nervous system that was running hot suddenly has nothing to push against.
The Chemical Crash
Endorphin withdrawal: Those natural opioids that made the pain feel transcendent? They recede. The comedown feels like low-grade opiate withdrawal—achiness, fatigue, emotional sensitivity. The body was numbing itself; now it isn't.
Adrenaline crash: Sustained stress hormone elevation followed by sudden drop. The same biochemistry that causes post-crisis exhaustion, shakiness, and emotional volatility. Your partner's body was prepared to fight a tiger; now it's wondering where the tiger went.
Oxytocin cliff: The bonding hormone surged during intimacy and contact. If that contact disappears abruptly, the withdrawal feels like abandonment—even if rationally they know you haven't abandoned them. The body doesn't do rational.
Cortisol rebound: Stress hormone that was suppressed during the endorphin high comes roaring back. This is the "48-hour flu"—the delayed crash that hits a day or two later when cortisol peaks in the absence of the other chemicals that were balancing it.
The Autonomic Cliff
Polyvagal theory frames this precisely. During scene, the nervous system is in high sympathetic activation—but held within a relational container that signals "safe." The ventral vagal system (social engagement, connection) co-regulates the sympathetic charge, making intensity feel exciting rather than terrifying.
Remove that container abruptly and the nervous system can flip into dorsal vagal—the shutdown response. This is the freeze state: dissociation, numbness, collapse, the body's last-resort response when threat plus no-escape. Drop isn't sadness. It's the nervous system slamming into emergency shutdown because the co-regulation that made the intensity survivable just vanished.
The scene pushed them to the edge. Aftercare is how they get back. Without it, they don't land—they crash.
The Application: The Recovery Protocol
Aftercare isn't one thing. It's a structured transition from high sympathetic activation back to parasympathetic baseline. The goal: ramp down the nervous system gently, maintain co-regulation through the chemical crash, signal safety continuously until the system stabilizes.
Immediate (0-15 minutes): The Soft Landing
Physical contact. Skin-to-skin if possible. C-tactile afferents—the nerves that register pleasant social touch—activate vagal pathways directly. Holding, stroking, wrapping them in your body heat. You're not cuddling; you're running a co-regulation protocol through their skin.
Warmth. Blankets, body heat, warm room. Temperature regulation goes haywire during sympathetic activation; they may be shivering even if the room is warm. External warmth signals safety to the autonomic system.
Breathing. Slow, audible breaths that they can entrain to. You're literally pacing their nervous system with your respiration. Extended exhales activate parasympathetic; if you breathe slowly, they'll start matching you without trying.
Voice. Low, slow, warm. Prosody carries autonomic state—your nervous system broadcasts through your voice. A calm voice is a co-regulation signal. Tell them they did well. Tell them they're safe. The content almost doesn't matter; the tone is doing the work.
Short-term (15-60 minutes): Restabilization
Glucose. Something sweet. Juice, chocolate, fruit. Intense scenes burn through blood sugar; the crash compounds the neurochemical crash. This isn't indulgence—it's metabolic support.
Hydration. Water, electrolytes. Stress hormones are dehydrating. Basic physiological restoration.
Continued presence. You don't have to do anything. Just be there. The oxytocin that spiked during connection needs continued connection to taper gradually instead of cliff-diving.
Light reality contact. Gentle questions that orient them to ordinary reality. "How are you feeling?" "Do you want more water?" You're bridging them back from scene-space to regular consciousness.
Extended (24-72 hours): The Delayed Crash
Check in. A text the next day. A call the day after that. The cortisol rebound often hits 24-48 hours post-scene—long after you've separated. Knowing someone is thinking about them, that the connection didn't end when the scene did, provides relational continuity through the delayed crash.
Normalize what's happening. "This is drop. It's normal. It's chemistry. It will pass." People in drop often think something is wrong with them. Naming the phenomenon reduces the secondary suffering of confusion and self-judgment.
Self-care scaffolding. Remind them: extra sleep, gentle food, nothing emotionally demanding for a day or two. They're in recovery. Treat it like recovery.
The Other Direction: Top Drop
Tops crash too. Different flavor, same neurochemistry.
Holding space for intense experience is work. Vigilance, attunement, responsibility, the sustained focus of keeping someone safe while pushing their edges. That's sympathetic activation plus cognitive load plus empathic attunement. When it ends, you crash too—often into guilt, doubt, exhaustion, or a strange flatness.
Tops need aftercare. This is the part nobody talks about. The person who just held the scene needs holding too. Touch, appreciation, acknowledgment of what they provided. "Thank you" is pharmacologically active when it comes from someone whose nervous system you just spent two hours attuning to.
If you're a bottom and you've never thought about your top's aftercare needs, think about it. If you're a top and you've been white-knuckling through post-scene crashes alone, stop. You deserve the protocol too.
The Through-Line
Fighter pilots get post-mission protocol. Surgeons scrub out with rituals. Athletes have cooldowns. Anyone who pushes human systems to their edges knows you don't just stop—you transition.
Intense erotic scenes push human systems to their edges. The neurochemistry is real: adrenaline, endorphins, oxytocin, cortisol surging and crashing. The autonomic dynamics are real: sympathetic redline to parasympathetic recovery, with dorsal shutdown waiting if the transition fails. This isn't psychology—it's physiology.
Aftercare is the transition protocol. Skin contact, warmth, breath, voice, glucose, presence, check-ins. Not because it's romantic. Not because you're supposed to. Because skipping it means handing someone a cortisol bomb with a 48-hour fuse and pretending you don't know what happens when it detonates.
You opened them up. You brought them somewhere intense. Now you bring them back.
That's not sweetness. That's engineering.
Substrate: Polyvagal Theory (Porges), Autonomic Neuroscience, Co-regulation Dynamics